


What the RUC: How Medicare’s Payment Reform Unraveled Primary Care


“In January 2025, Governor Maura Healey signed Chapter 343 of the Acts of 2024… establishes a new 25-member task force on primary care access, delivery, and financial sustainability in the Commonwealth,” https://masshpc.gov/offices-and-task-forces/pctf#StayConnected
I’m honored to represent the Massachusetts League of Community Health Centers on the state’s “Primary Care Access, Delivery, and Payment Task Force.” In preparation for this role, I’ve been reviewing the history of primary care reform attempts and will share my findings with you.
The American healthcare system is often described as complex, expensive, and inequitable. At the center of this system lies an obscure but powerful committee that most Americans have never heard of — the Relative Value Scale Update Committee, or “the RUC” (pronounced “ruck”). This little-known group of physicians wields enormous influence over how healthcare is paid for in America, directly affecting which medical specialties thrive, who enters primary care, and ultimately, how our healthcare dollars are spent.
The RUC was created with noble intentions: to help balance a healthcare system that undervalued cognitive services (like primary care office visits) compared to procedures (like surgeries). Yet over time, the mechanism designed to correct these disparities has instead reinforced them — contributing to our current crisis in primary care access, rising healthcare costs, and specialist-heavy system.
Private insurers typically follow Medicare’s lead on payment rates by using the Medicare fee schedule as their baseline, often paying a percentage above the Medicare rates. The RUC’s influence extends beyond Medicare because commercial payers generally adopt the exact RVU valuations that Medicare uses, sometimes with different conversion factors, making the RUC’s decisions effectively the standard for nearly all physician payments throughout the American healthcare system.
Let’s explore how a well-intentioned policy solution went astray, the consequences for our healthcare system, and potential paths forward.
The Birth of RBRVS: A Solution to Inequity
To understand the RUC, we must first understand the problem it was created to solve.
In the 1980s, the “usual, customary, and reasonable” (UCR) payment system for Medicare had created significant disparities between the incomes of procedural specialists and primary care physicians. This payment approach allowed doctors to set their own fees, which Medicare would pay. As physician and health policy expert Bob Berenson explained, “It was basically an honor system where doctors billed what they thought was appropriate, and Medicare generally paid it.”
By the mid-1980s, policy experts recognized this approach was unsustainable — it was driving up costs and creating perverse incentives. More critically, it was contributing to a serious imbalance:
Procedural specialists (surgeons, cardiologists, etc.) could earn multiples of what primary care doctors earned
Medical students were increasingly avoiding primary care due to income disparities
Healthcare costs were spiraling upward with no rational basis for many fees
In response, Congress mandated the development of a Resource-Based Relative Value Scale (RBRVS) system as part of broader Medicare reforms. The Harvard team led by economist William Hsiao conducted a rigorous study that aimed to quantify the relative value of different physician services based on:
Time spent before, during, and after procedures or visits
Mental effort and judgment required
Technical skill and physical effort
Stress involved in caring for the patient
Resources needed to provide the service
The Hsiao study was comprehensive. It involved thousands of physicians across specialties, used cross-specialty validation panels, and employed sophisticated methodology to objectively determine the relative “work” involved in different medical services. When completed, the study recommended dramatic shifts in payment — boosting cognitive services like office visits by 60–70% while reducing some procedural specialties’ payments by 40–50%.
As the Health Policy Commission report notes: “This was not guesswork, but rather a rigorous, multispecialty, large-scale study involving 3,200 surveyed physicians and 18 specialty societies that cross-validated each other’s data.”
The Initial Win for Primary Care
When the RBRVS system was implemented through the Omnibus Budget Reconciliation Act of 1989 (OBRA-89), the impact was initially positive for primary care. As the implementation gradually phased in between 1992 and 1996:
Family physicians saw Medicare payments increase by approximately 36%
Some procedural specialists saw significant reductions
The income gap between cognitive and procedural specialties began to narrow
This was arguably the high-water mark for primary care’s standing in Medicare payment policy. The RBRVS system worked as designed, correcting historical imbalances and creating a more level playing field.
As the Health Policy Commission report states: “RBRVS initially worked as intended, correcting some of the extreme payment disparities between procedural and cognitive work.”
Enter the RUC: A Fateful Decision
Here’s where our story takes its critical turn.
The RBRVS system needed regular updates to account for new procedures, changes in practice patterns, and evolving technology. Instead of housing this updating process within a government agency or an independent body, the Centers for Medicare and Medicaid Services (CMS, then called HCFA) accepted a proposal from the American Medical Association (AMA) to create a physician-led committee to handle these updates.
In 1991, the RUC was born — officially named the AMA/Specialty Society Relative Value Scale Update Committee.
This fateful decision effectively gave the medical profession control over its own payment rates. While seemingly reasonable — who better to determine physician work than physicians themselves? — it created an inherent conflict of interest and set the stage for the gradual undoing of the RBRVS system’s equity goals.
The original RUC structure was telling:
29 members, predominantly specialists (reflecting the specialty-heavy composition of organized medicine)
Closed-door meetings with limited transparency
Dominated by procedural specialists who had the most to lose from the RBRVS reforms
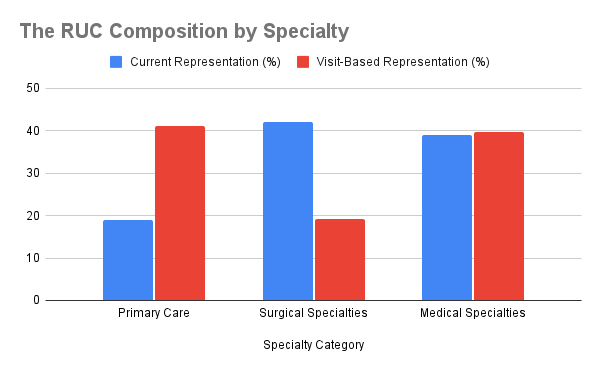
As economist Uwe Reinhardt later observed, the arrangement was like “putting the fox in charge of the henhouse.” The RUC’s composition fundamentally misrepresents the actual distribution of healthcare delivery in America, with primary care physicians holding only about 15% of the committee’s seats despite primary care accounting for 40–60% of all outpatient visits nationwide. This structural imbalance creates a system where the voices making decisions about payment values dramatically underrepresent the very specialties that serve as the foundation for most Americans’ healthcare experiences.
The Critical Issue: Beyond Physician Income
What’s often lost in discussions about the RUC is that the problem isn’t simply about physician income disparities. It’s about the broader sustainability of primary care as a system and the critical need for team-based care. The issue isn’t just that primary care physicians are underpaid compared to specialists (though they are), but that the entire primary care ecosystem is underfunded, and as such unsustainable in its current state.
The RBRVS and RUC systems don’t adequately recognize a fundamental truth about primary care: a large portion of practice costs are fixed overhead expenses. The 1988 Hsiao study analyzed in the Becker, Dunn, and Hsiao paper concluded that:
“Among most specialties, the range of relative practice costs as a percentage of gross revenue is approximately 15%. Four specialties fall outside this range: pathology, psychiatry, rheumatology, and orthopedic surgery.”
For primary care practices, these fixed costs represent approximately 60–65% of their total expenses. This includes office space, equipment, electronic health record systems, and support staff. When reimbursement is inadequate, practices cannot afford to hire the necessary team members:
Care managers to coordinate complex patient needs
Scribes to reduce documentation burden
Behavioral health specialists for integrated care
Nurses and medical assistants to support comprehensive care
As the Health Policy Commission report notes, primary care physicians simply cannot provide high-quality care without adequate support: “Research has found that providing evidence-based primary care without an adequate care team requires nearly 27 hours of work per day.”
The Gradual Erosion: How the RUC Transformed RBRVS
Over the next decade, several dynamics played out that gradually eroded the initial equity gains:
1. Specialty Dominance in the Process
The RUC voting membership remained dominated by procedural specialties. Primary care specialties like family medicine and internal medicine represented a small minority of votes, despite serving as the entry point for most patients.
As noted in the Health Policy Commission report: “The RUC’s specialty-driven valuations systematically favored procedures, contributing to a growing income gap once again.”
2. The Survey Methodology Problem
The RUC relies on specialty societies to conduct surveys of their own members to determine how much “work” is involved in various procedures. This created clear incentives for inflation — what specialty would argue that its procedures should be paid less?
The Government Accountability Office (GAO) highlighted that by 2009, surveys often included fewer than 50 physicians — often hand-selected by specialty societies. Meanwhile, primary care services like office visits weren’t systematically reviewed for over a decade.
3. CMS Deference
Most critically, CMS accepted the vast majority of RUC recommendations — over 90% of them historically. This remarkable deference effectively ceded control of the fee schedule to the RUC.
As the Health Policy Commission report observes: “By 2005, CMS was formally accepting 92% of RUC recommendations for work RVUs. This was not a passive act — it reflected CMS’s structural dependence on RUC-generated data.”
4. New Technology Coding and Valuation
Technological advances led to constantly creating new procedure codes, each requiring RUC valuation. Procedural specialists aggressively pursued new codes and high valuations for new technologies. Meanwhile, the core office visit codes for primary care remained largely static.
The Administrative Burden Cycle
One of the most damaging aspects of this system has been the creation of what might be called “the administrative burden cycle” in primary care:
Inadequate Reimbursement: Primary care services are undervalued relative to procedures, providing less revenue.
Insufficient Team Support: Without adequate revenue, practices cannot afford to hire the support staff needed for team-based care.
Increased Physician Administrative Burden: Without proper support, physicians must handle more administrative tasks themselves, from documentation to prior authorizations.
Reduced Patient Time: As physicians spend more time on administrative work, they have less time for direct patient care.
Increased Visit Volume: To maintain practice revenue, primary care physicians must see more patients in less time.
Lower Job Satisfaction: The combination of high administrative burden, insufficient support, and rushed patient encounters leads to burnout.
Workforce Attrition: Physicians reduce hours or leave primary care entirely, worsening access problems.
As the Health Policy Commission report shows, Massachusetts physicians report alarming levels of burnout: “55% of physicians surveyed experienced symptoms of burnout…More than half of respondents already had reduced their clinical hours or planned to in the next 12 months.”
The “Procedural Rebound” Phase: 1995–2005
By the early 2000s, something remarkable had happened — the exact opposite of what RBRVS was designed to achieve. Primary care’s initial gains were largely erased, while procedural specialists had not only recovered but often exceeded their pre-RBRVS incomes.
This period, which might be called the “procedural rebound,” had several key features:
RUC-Driven Code Inflation: Procedural specialists drove the creation and valuation of hundreds of new codes, often at high RVU values.
Stagnant E&M Codes: While procedure codes proliferated, the evaluation and management (E&M) codes that primary care physicians primarily bill remained largely unchanged.
Volume Growth in Procedures: The financial incentives encouraged growth in procedural volume, while primary care visit length remained constrained.
Widening Income Gap: The doctor income gap that RBRVS was designed to narrow began widening again.
As Dr. John Goodson noted in his influential 2007 JAMA article, “Medicine’s generalist base is disappearing as a consequence of the reimbursement system crafted to save it — the resource-based relative value scale.”
The Consequences: A Primary Care System in Crisis
The impact of these payment distortions has been profound:
Workforce Distortions: Medical students increasingly chose specialty careers over primary care. Massachusetts now has among the lowest shares of new physicians entering primary care in the nation, with only 1 in 7 new physicians entering primary care as of 2021.
Care Access Problems: As the Health Policy Commission report notes, “Boston had the second-longest wait times for a new patient appointment for a physical in 2022” among 15 major metro areas.
Primary Care Spending Decline: Primary care declined as a percentage of all commercial spending in Massachusetts between 2017 and 2022, from 8.4% to 7.5%.
Unsustainable Workload: Primary care physicians face overwhelming administrative burden and patient panel sizes, leading to burnout and early retirement.
Rising Healthcare Costs: With primary care undervalued, patients end up in more expensive care settings, including emergency departments. Roughly 40% of emergency department visits in Massachusetts are for conditions that could have been treated in primary care.
In 2021, the United States allocated a mere 4.7% of its total healthcare spending to primary care, a stark contrast to the average of 14% observed in other high-income nations.
Recent Reform Efforts: Too Little, Too Late?
Recognizing these problems, there have been some efforts to reform the RUC and rebalance payment:
Addition of Primary Care Seats: In 2012, the RUC expanded to 31 members, adding seats for geriatrics and a rotating primary care position. However, proceduralists still maintained a strong majority.
E&M Code Revaluation: In 2021, a significant update to office visit codes increased payment for primary care services — the most substantial revaluation since RBRVS began.
State-Level Reforms: Several states have set primary care spending targets, including Rhode Island (10.7% of total healthcare spending), Oregon (12%), and Washington (12%).
Alternative Payment Models: The growth of value-based payment has created new incentives that may better reward primary care’s coordination role.
However, the fundamental problems with the RUC process remain largely unaddressed. The committee still operates with limited transparency, specialty dominance, and inherent conflicts of interest.
The Team-Based Care Solution
Meaningful reform isn’t just about paying primary care physicians more — it’s about creating payment models that support the entire primary care ecosystem. What’s needed is:
Adequate Funding for Team-Based Care: Payment models that provide enough revenue to hire and retain a full team of care providers, not just the physician.
Reduced Administrative Burden: Systems that allow physicians to focus on clinical decision-making rather than documentation and insurance requirements.
Capitation Over Fee-for-Service: Moving away from visit-based payment to per-patient paymenthamster wheel of FFS, allowing practices to innovate in delivering care and creating greater access to patient care.
Recognition of Care Complexity: Payment systems that account for the increasing complexity of primary care patients, many with multiple chronic conditions.
As the Health Policy Commission report highlights: “Promising aspects of new care models could likely be replicated in traditional practices with greater use of capitated funding so practices can invest in support staff and clinician activities that are not reimbursable under fee-for-service payment.”

Massachusetts Takes Action
Massachusetts has recognized the urgent need for primary care reform. In 2024, the state established a Primary Care Payment and Delivery Task Force through Section 80 of Chapter 343 of the Acts of 2024. This 25-member task force is charged with addressing key issues:
Defining primary care services, codes, and providers
Developing standardized data reporting requirements
Establishing a primary care spending target
Proposing new payment models to increase reimbursement
Assessing the impact of health plan design on access and equity
Creating workforce development plans
The task force must deliver its recommendations by mid-2026, with interim reports beginning in September 2025.
The Path Forward: Reclaiming the Original Vision
What would it take to return to the original intention of the RBRVS system? Several potential reforms emerge:
Independent Valuation: Removing the conflict of interest by creating a truly independent body to update the RBRVS, perhaps modeled on MedPAC or the Medicare Evidence Development & Coverage Advisory Committee.
Transparency Requirements: Mandating full transparency for the RUC process, including public meetings, detailed voting records, and release of survey data.
Primary Care Spending Targets: Following the lead of states like Rhode Island and Oregon in establishing minimum primary care spending percentages.
Capitation and Alternative Payment: Moving away from reliance on fee-for-service toward alternative payment models that better reward primary care’s coordination role.
Administrative Burden Reduction: Addressing the unsustainable administrative work that has made primary care increasingly challenging to practice.
The story of the RUC illustrates a classic case of “regulatory capture” — where the regulated entities gain control of the regulatory process. The RUC was created with the intention of maintaining the equity gains of the RBRVS system, but instead became the mechanism by which those gains were gradually eroded.
The solution isn’t simply to pay primary care physicians more, though that’s certainly needed. It is about fundamentally reforming payment to support team-based care. When primary care practices receive adequate funding, they can provide the full spectrum of services patients need—not just physician visits but care coordination, behavioral health integration, health coaching, and more.
Only with such comprehensive reform can we hope to rebuild a primary care system that serves as the foundation for high-quality, accessible healthcare for all — one where physicians can focus on caring for patients rather than struggling with administrative burdens due to inadequate practice resources.
As Massachusetts and other states continue to address these challenges, understanding the historical roots of our current payment problems is essential. Lessons are either learned or repeated. The RUC may be little-known, but its influence on our healthcare system has been devastating; an iatrogenic malady that began as a well-intended treatment. We can and must do better; our patients deserve better. Reforming this broken payment system isn’t just an economic imperative — it’s a moral one, essential to restoring the foundation of healthcare that millions of Americans depend on every day.
Stay tuned for the next installment in the series, where we’ll examine HMO capitation reform
It promised to transform primary care physicians into the quarterbacks of healthcare, calling the plays and coordinating the team. Instead, it turned them into the healthcare system’s loss leaders — valuable enough to draw patients through the door, but priced below cost, with health systems hoping to recover on the “high-margin items” down the specialist hallway.
From clipboard to chopping block: how primary care became the practice that pays for everything but itself.
Sources:
Massachusetts Health Policy Commission. “RUC Primary Care Disadvantage Exploration.” 2024.
Massachusetts Health Policy Commission. “A Dire Diagnosis: The Declining Health of Primary Care in Massachusetts and the Urgent Need for Action.” January 2025.
Section 80 of Chapter 343 of the Acts of 2024, establishing the Primary Care Payment and Delivery Task Force.
Goodson JD. “Unintended Consequences of Resource-Based Relative Value Scale Reimbursement.” JAMA. 2007;298(19):2308–2310.
Government Accountability Office. “Medicare Physician Payments: CMS Should Improve the Accuracy of Work Relative Value Units Used to Set Physician Payments.” GAO-09–647, July 2009.
Becker ER, Dunn D, Hsiao WC. “Relative Cost Differences Among Physicians’ Specialty Practices.” JAMA. 1988;260:2397–2402
Milbank Memorial Fund Report
Kravet, S., Hoang, D., Bazemore, A., & Jabbarpour, Y. (2024). The health of U.S. primary care: 2024 scorecard report — No one can see you now. Milbank Memorial Fund. Retrieved from https://www.milbank.org/publications/the-health-of-us-primary-care-2024-scorecard-report-no-one-can-see-you-now/Commonwealth Fund Report
Shah, A., Schneider, E. C., & Tikkanen, R. (2024). Finger on the pulse: Primary care in the U.S. and nine other countries. The Commonwealth Fund. Retrieved from https://www.commonwealthfund.org/publications/issue-briefs/2024/mar/finger-on-pulse-primary-care-us-nine-countries

Written by Renee Crichlow MD, Health Policy & Healthcare AI
Leading a charge in the fight to fix healthcare through practice redesign, payment reform, & primary care workforce A national health policy in AI expert